Welcome to our Tips and Tricks Resource
You can scroll down to read the whole page, or click on the links below to skip directly to that section.
- Staying positive
- Ask lots of questions
- Ask for what you need
- Trust your instincts and knowledge
- Managing other people’s reactions
- Tube re-insertions at hospital
- Taping
- Feeding on the go
- Siblings of tube-fed kids
We’re getting our videos ready to share! In the meantime, watch Irene talk about what she takes with her when she leaves the house with her son Connor.
Staying positive
Parenting is hard enough as it is. With the added complexity of feeding difficulties, it’s easy to feel overwhelmed and to miss out on the many joys and delights that will still be there.
Click here to read more…
Taking photos, marking the experience, and accepting that ‘it is what it is’ rather than fighting the idea of tube-feeding all helped other parents stay positive.
Taking, sharing and enjoying photos of your child while wearing a tube can be a great way to overcome negative feelings about how the tube looks and the whole idea of tube-feeding. This was an important part of Siân staying positive about her daughter Tori’s development – see their Real Story for more and all their ups and downs.
Roberta found this was incredibly important, but needed some managing with the grandparents. We asked her if having a tube affected how she took photos of Eliza. This is what she had to say.
No. Because this is her story. This is how I felt. Eliza has a story, when she’s older she’s not going to have this tube, it’s only a short term thing. This is part of her story. She pulled the tube out and I took a picture and I was like, oh my god, this is the first time that I’ve seen her full face. Then we took a photo and I was like, take photos, take photos, just so I can tell her about it. My mum actually got the photo printed out and put it in her house, because there was no tube. I told her off for it. Because that’s not her story. Why can’t she have photos in the house with the tube? Because that’s her story.
Roberta
Julia suggested making a necklace, where each bead represents something that happened on your tube-feeding journey. It could one bead each time they pull the tube out (that could get quite long quite quickly), or for each 100g they gain in weight, or even each time you get something wrong with the tube-feeding!
Tube-feeding can be scary and daunting. When you are in the thick of it, especially in the early days, it’s hard to get some perspective and see it in relation to other things that matter more. Freya told us how she went from panic to acceptance:
I think at the end of the day, all will be okay. I think we panic and whatnot, but there are worse situations than tube feeding. Do you know what I mean? As long as the other aspects, them growing, their development, if that’s all good, this is really, really minor and you can get control over it. Because this is our norm. You think the tube is such a pain in the arse that you just want to get it out. But it’s not the tube or anything like that that you have a problem with, you don’t care. You just want your kid to develop and be healthy and whatnot. I think it all starts from the day they’re born, if they’ve got their feeding tube and you recognise that and you’re aware of it more and you’re like, you know what, that’s that, I’m going to accept that and that’s what it is.
Freya
The getting the balance right section has more from parents about giving tube-feeding the serious attention it deserves, but not letting it take over everything.
Learning all the things other parents think are helpful to know might also be useful in staying positive because they make the whole tube-feeding hoo-ha seem more normal and manageable.
Tell us how you are staying positive. Are you marking your journey, taking photos, or doing something else that other parents might find useful?
Ask lots of questions
Asking questions is much better than being left not knowing what to do, without the help you need, or unaware of the options available – it’s a key way of keeping negative thoughts at bay and avoiding a slump where things get too much.
Click here to read more…
Lisa’s son Henry was vomiting a lot. Asking a nurse helped her understand what was going on, and made her much less worried:
One of the things with having kids with a feeding tube, is that if they’re sick, they vomit a lot. That’s very important to know, because I used to think, why is he always vomiting? Because he always had bronchiolitis, this kid was vomiting all his feeds constantly. I didn’t know that at the beginning. Then I asked one of the nurses about it and she assured me, this is normal – for some reason they find that they vomit excessively when they’re really sick and that’s what’s happened to him. It was really bad because his weight was already low and he’s vomiting all his feeds all the time. That’s another reason why I’m all for the PEG, because he’s not sick, he’s not vomiting, which means he’s putting on weight. Whereas before he was always underweight.
[Audio – Lisa:TT-A-1]
(You can explore more about getting a PEG in our To PEG or not section)
Mandy only found out there was a day-care that could take a tube-fed child by asking a nurse. This meant she could go back to work.
I ask questions, I’m nosy. I asked about going back to work when your child is still tube-feeding. I asked the nurse and she told me that there’s a number of parents that have gone back to work and there’s – especially in my area, that there is one day care that knows really well how to do it. Because one of the ladies’ daughter had a feeding tube, so she knows how to do it. But also that they’ve gotten the nurses out there to train. So it’s possible. If I didn’t ask that question, I wouldn’t have known.
Mandy
Some other things you could ask about include:
- how long the tube might be needed for – lots of parents thought it wold be a few weeks and found it went on for much longer
- seeking playgroups specifically set up for tube-feeding
There’s one near me, at the Community Centre, for kids that have a tube, kids that are delayed so they can get in for an hour or two with kids like them”
Rhona
- whether day-care providers if they would be willing for you to teach them how to do a tube feed (see Ruth’s Real Story)
- whether you could be trained to re-insert an NG tube
- what the options for having a PEG might be (see To PEG or not)
He had an NG tube until he was nine months old, and then surprise, surprise! I discovered another type of feeding tube, a G-tube (or PEG), which I had no idea about. I would have loved to have known the options early on.
Hannah
Read more about Hannah and Tony in their Real Story
Ask for what you need
The people helping might not know what matters to you, or what works best for you and your child, so if there’s something specific you need, ask for it.
Click here to read more…
Shannon found the standard tape she was given at hospital didn’t stick well on her son’s skin. So she asked for alternatives – and needed to be persistent.
“At the hospital, my experience would be the tape comes off and it’s shit. So then I would say, this is no good, do you have another tape that we could try? I would keep on doing that and then we found one that was good – a special tape that from another ward, every time I used to go there, I used to request it, because that one would be the best for his skin. Then every time I would come I’d say, I want this tape, and they would get it from another ward. But then it got to a point where they ran out, they said we don’t have any more. So I researched on my phone and found a supplier that sells it and we bought it for him. I need that tape because he’s got bad skin, any other tape and he would have blisters.”
Shannon
There’s more about taping below.
Trust your instincts and your knowledge as a parent
Click here to read the Video Transcript instead
“I keep his hands occupied. We feed him in front of the TV. Not every day, but in front of his favourite shows, just to keep him – and that’s probably one little tip. I was told not to do that, because he’s not associating feeding with mouth and that kind of stuff and his tummy’s full and that kind of – and that’s fine, medically, I completely get it, but when you’re there, trying to hold the tube, hold him down, make sure he doesn’t pull anything, when the extension is – it’s a tube that you connect. That’s when it’s a little bit more sensitive, because he can pull that and rip it out of his tummy. So, there’s safety precautions that you’ve got to take. So, I feed him and him bent over in his high chair – he’s better off laying flat. They’re the types of things that I wish I’d known. I discovered okay, we’re home, we’ve got to do what works for us, whereas if another parent had said to me hey, you know what? If you need to feed him in front of the TV, put on his favourite show, and two out of the six feeds are doing that, or three out of the six feeds are doing that, it’s not going to break his association. It’s okay. Getting the calories in is way more important, and making it enjoyable, so give him his food when he’s not preoccupied with it, when you’re not preoccupied with it. Sit at family meals and make his oral feeding the enjoyment and leave the tube feeding for nutrition. Another parent told me that.”
As a parent, you know your child better than anyone else in the world. You also know what is important to you. Nearly all parents find it hard to trust their instincts sometimes, and this can be even more difficult when there are feeding difficulties.
Click here to read more…
“At the end of the day a baby is a baby and a child is a child. At the end of the day, you as a mother or a parent or whatever know exactly. You have an instinct, you have a feeling of some sort, you’ve just got to follow it.”
Adam
This can sometimes mean being ready to question advice from professionals if you’re finding it isn’t working for you. Kitty listened to her instincts and did what she thought Geoffrey needed, even though this meant not following the guidance she had been given:
“I think it’s important to actually read your child. As a mother, even though your child is going through all this hoo-ha, you’ve got something in there, listen to yourself. With Geoffrey, they would tell me to put him in a certain position to feed him with the bottle first, before I started tube feeding her. I noticed when we got home, yes, it was working, but at one point it started not to work. He wanted to be lying down on her back, like elevated slightly up. Then we started doing that and then he started taking the bottle a little bit more. It was just all about reading him and what he wants. Because even though it’s a different circumstance to your first one or whatever, or if it is your first child and you have to go through this hoo-ha, you really need to just listen to yourself and your instincts. Believe it or not, it’s the right one. With the advice of nurses and doctors and everything all into that, you will make the right decision and all will be, at the end of the day, okay.”
Kitty
The best clinicians in the world cannot guarantee that their suggestions will work for you and your child. Dee found that the feeding routine needed to be adapted to suit her child. She was careful and didn’t make drastic changes, and talked about it with her care team later.
“I’ve met with the team, and it’s not working. You keep on trying and you’re going crazy, it’s not working. Then all of a sudden you think, let me try this, and I’ve tried it and it works. Obviously you’re not going to go changing completely something, but my routine now when I’m offering the feed compared to when I was offering it before it’s working much better. Just something so small that’s minor but it’s made a difference.”
Dee
Hannah found that what worked for her contradicted some of the advice she had about feeding associations. She trusted her own instincts but also was open to suggestions from other parents, too:
You can read more about Hannah and her family in their Real Story.
Just like parents, staff in hospitals sometimes get it wrong, too. If you’re concerned about something, be confident to say so, and make sure any potential confusion or miscommunication is cleared up. Janet told us how the prospect of being sent home too early was quite scary, but quickly resolved.
“One thing that they got wrong was this nurse manager came up to me and she said, oh, you’re ready to go home. At this point I hadn’t done any training. I started panicking, what is going on? Last time I spoke to someone, they told me something different. So I had a panic, and then I mentioned it during the walk-around when the doctor comes. They, no, she’s not going home, they’re not ready, the baby is not even eating. She was actually going to send me home without a tube. This kid’s not eating. How can I go home without a tube? It just doesn’t make sense. Anyway, the doctor stepped in and that’s when I got the training and everything else. The nurse manager then came back and she apologised.”
Janet
Managing other people’s reactions to a child with a feeding tube
Many people haven’t seen a tube-fed child before, and don’t really know how to react. Expecting questions and comments from curious (but not always helpful or welcome) strangers is a good start (see what to expect).
Even better is to have some strategies that you use so you don’t have to think up how to respond on the spot.
Click here to read more…
Here’s how Naomi deals with people who aren’t sure what to think:
“Straight up I just say, it’s a feeding tube. That’s it. It’s as simple as that, because they think my child is dying and it can’t breathe and they go to this whole other level. Obviously there’s more to her story, but I just say, it’s a feeding tube, she was a premmie, and that’s it. As soon as they hear premmie and feeding, they’re at ease with it, they’re like, oh, how nice, that’s lovely, she’s a good size, she’s fine.”
Naomi
Naomi
Read how Hannah deals with curious onlookers in the ‘Feeding on the go’ section below.
Tube Re-insertions in Hospital
It’s pretty much inevitable that your child will pull her or his NG tube out. Probably many times! (see What to expect). Sometimes, it’s possible to get trained do re-insert the tube yourself (see Tips and Tricks), but even then, there’s usually a period before that when a tube being pulled out means a trip to hospital to have it put back in.
Click here to read more…
Fatima said it helped her to call the hospital in advance to time the visit to get seen quickly
“See if they’re available and fit in with their rounds, because if they’re busy, they’re not going to do it for you, and when you get there you’ve got to wait.”
Fatima
Fatima
Often, things will go smoothly, but not everyone who helps you in hospital will be as knowledgeable as you about tube-feeding. They might need your help to get things right.
Tracey describes how she had to put her foot down in hospital to get an appropriate tube, and then again because she knew the NG tube wasn’t in correctly:
“Maybe they weren’t trained or hadn’t done it before or for a long time. They kept on getting the wrong tube down from the ward. So they would come back with an adult tube, then a bigger tube – we would show them and tell them what size it was. I don’t know what they were doing, but they came back with four or five tubes. When they put the tube in his nose, because they hadn’t done it before, they had shoved it all in here, in his sinuses. Then they gave him back to me, he was crying, I was trying to aspirate, but couldn’t aspirate. I was like, there’s something wrong, I can’t get anything, we can’t feed him. They said, do you want to give him a little bit? I said, no, no, no, I can’t aspirate. Aspirating is when the tube is in the right place, you can get some acid out of the stomach and you do a little test. To us it’s simple, but to them it’s not because maybe they haven’t done it before.”
racey
racey
Taping and looking after your child’s facial skin
Taping an NG tube in place and looking after the facial skin are important, but tricky. There’s no one approach that suits every child. Their heads are different shapes, their skin reacts differently to tape.
Click here to read more…
Cory tried to minimise the gaps where the tube wasn’t taped down, to make it harder for Jenn to pull the tube out. While some ways of taping work better than others, nothing is 100% child-proof! (There’s more in Cory’s full Real Story).
Listen to Cory describe his taping experience:
[Transcript]
I do a whole strip of tape, literally from her nose or her cheek all the way to her ear. So it’s just only this little bit here by her nostrils where she can pull it out. She’s always trying to. There’s that slight little gap between your cheek there and your nose, and that’s where she goes for it. She’ll get in there, even though I’m taping it. She’ll get that little finger of hers and just go bung, and then it’s all over. If it’s just a little bit out, then I usually kind of just put it back in. But if she’s ripped the whole thing out, forget about it. It’s really hard. Because she’s got oily skin, it doesn’t – there’s not a good enough tape, to be honest with you, nothing really holds it down properly, I’ve found.
Another issue is when to change the tape. Changing it often can irritate the skin and be annoying for your child. But leaving it on too long isn’t good either as it can come unstuck and get dirty. There are no hard and fast rules about how often to replace the tape. Here’s what Grace did:
We tend to the change the taping maybe every three days. It just gets really brown and it just doesn’t look pretty. They just say change the tape whenever you need to, really. They don’t really give you a timeframe of when to change it. Obviously because when you’re bathing and things like that, you’re washing your face and whatnot, and that tape slowly starts to curl up and that’s how it all kind of starts. So that’s when I change it.
Grace
Grace
Kalpana told us how she cut big pieces of tape like Cory did, and could leave the tape on longer, provided it was the right tape for her son’s skin:
I changed mine because of his skin, but if his skin was okay, I wouldn’t change it. If I used the hospital tape, by the time I got home, about five hours later, I’d need to change it. That’s how terrible that tape was. I could leave mine for a long time. I bought tape with pictures, there’s little cars and things like that, and I used to put that on. I used to cut around the picture, that would take a larger space of his cheek. Because that was larger, it used to stick on better onto his cheek, so there was never that opportunity for him to pull it or rip, and it used to go further out.
[Audio – Kalpana:TT-A-1]
[Audio – Kalpana:TT-A-1]
Siân (who you can read more about in the Real Stories section) shared these great tips on taping:
Distraction, and having everything ready to go. Knowing how much tape you need, how much time you need. The length of tape, keeping your measurement right. I change it when it’s looking really disgusting. You can try and add little bits here and there to stop having to take the whole thing off, and patch it up.
Siân
Siân
Hannah ended up feeling that getting taping right was one of the most important things to figure out, because it affected so many other things. Here is her detailed description of what she and her husband found worked for their boy Tony:
We put the skin barrier underneath, the DuoDERM on top, the tube in between, and the brown tape over it, so his skin was not affected. Yes, it was irritated because something was there, but it wasn’t affected because we barriered it up, then the waterproof film on top. It wasn’t bulky because everything was very, very fine. We could go a week without changing it, except when he vomited or when snot got caught underneath. The NGT didn’t stop him swimming, though we took care to avoid his face getting splashed.
Hannah
Hannah
You can read more about Hannah and her family in their Real Story.
Shannon found that hospitals often had other kinds of tape, but she needed to ask for it. In the end, she found a supplier and bought a load of the tape that suited her son best (see Ask for what you need).
Yolanda found that the bacterial wipe was a bit harsh for her daughter’s skin, making it go bright red, so she started using water instead. This is another example of sometimes having to figure things out as you go along – learning from trial and error is part of what to expect as a parent of a tube-fed child.
Other tips we heard about included using Ruth’s way of using little jewellery bags you can get from a two-dollar shop, rolling them up and feeding any excess tube in, tucking it down the back of their t-shirt. That way it feels less like the baby has a strangulation device attached to them! (Ruth’s is one of the Real Stories).
Feeding on the go
How on Earth can you feed your child using a tube while out and about? In the car? In a café? Even while walking with a pram? Each family finds its own way to manage these things, but the most important thing is: it is possible!
Click here to read more…
A common tip is to re-purpose things that are cheap and easily available, but make a big difference to tube-feeding. Several parents found that a fabric hanger that could be used to hold TV remote controls or go over the edge of a cot was fantastic for storing a pump and making it easy to transport.
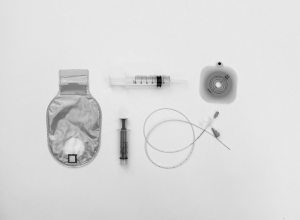
Another thing lots of parents did was create their own packing list or a checklist for when they went out, so they didn’t leave something like extra tape, the pH stick, adapters for the pump, a spare NG tube or the syringe at home. Do you have your own checklist? Share it with us through Your Story.
Here’s how Jasmine does a feed while out with her son in his pram:
“I got to a point, say if I was out and he needed a feed, let’s say if I was shopping or something, I had a cup holder for holding your coffee or bottles of water or whatever, so I would put that in a cup holder and I would feed him while pushing a pram. Then I’ll stop it when I’m done and, he would get fed as I’m pushing the pram. At one stage, he would vomit if he was sitting up, so with the pram, you can adjust it so he can sit up or lie down. However you want to feed him, you can do it. I just have it in the cup holder, all I have to do is just keep an eye on him, just in case he’s choking or anything like that, but that’s about it. Other parents have got other tactics that they use to feed them.”
Jasmine
Jasmine
Jonny and Siân made feeding Tori with an NG tube away from home work for them:
“We never really dwelled on the tube. Of course, Tori took priority with feeding and all that stuff, but we wanted to keep the routine as normal as possible. So we did just kind of get out there and if we had to feed on the go, we fed on the go. We had Velcro strapped inside the car to feed if we were feeding in the car, or multiple syringes in handbags in case we had to do that. We had a back-up tape kit in case the tape came off, and a spare NG tube in the glovebox of the car in case she pulled it out while we were out and about and we had to go to the hospital. It’s just preparation and knowing that if we needed to get out and do that normal life stuff, we were ready to go. It’s about finding that balance between normal life and the life you have with an NG baby.”
Sian
Sian
Read more about Jonny and Siân’s experience in their Real Story.
Tube-feeding on the go isn’t just about being out and about near home. Nicole’s son Jasper used an NG tube for two and half years (see To PEG or not for more about her decision not to switch to a PEG). During this time they went on holiday, and she described how they made this work:
“I remember we went away on holiday and we took the little chair that I used to feed Jasper in. I had this contraption – chopsticks tied with elastic bands. Goodness only knows what people must have thought! It’s to keep the gravity feed up. You just become expert. I worked at how to attach everything to the pram, just to have it so it wasn’t going to spill.”
Nicole
Nicole
A big part of feeding while out and about involves how others around you respond. There’s not much you can do to avoid people having a look, so Hannah had this advice:
“You want to look? Have a look! You’ll find most people won’t actually say anything, they just look. You have to have your own confidence. Accept the baby is tube-fed and accept yourself. You have to accept, and then you don’t really mind. If people want to look, they can look. People can think what they think, but you have to accept yourself, your baby is tube-fed. You have to build up your confidence, emotionally, but then if people want to look, go ahead and look.”
Hannah
Hannah
There’s more about managing the public in this section, and more about Hannah’s experience in her full Real Story.
Siblings of tube-fed kids
Getting siblings involved in feeding
One of things to expect is that any siblings of a tube-fed child will be very aware and curious, and will want to be involved. Giving them a positive, active role in the tube-feeding process can be fun for them, help to develop sibling bonds, and avoid some of the issues of attention being diverted away from the sibling. It can also ensure they see the tubes as something normal, not something to be scared of or worried about.
Click here to read more…
Many parents realised that their other children were actually more alert and capable in relation to tube-feeding than they first thought. Juan, father of Leo and his older brother, explained:
“Getting them involved, explaining it to them, you think that they’re not going to understand, but they do somehow. Then seeing you doing it all the time and you saying – because you know, as kids, they start to copy you as well. You say, don’t touch the tube, Leo, or, don’t pull out the tube, Leo. Because they hear all of that, and because they hear that, then they start saying the same thing as well. So that’s as well another way in how they learn everything.”
Juan
Juan
Tina’s way of involving Ava in feeding Tyler gave the daughter lots to do and made her feel important:
“I would take Ava for one of the feedings and she would be a part of it. She’d sit next to me and we’d talk or we’d sing to Tyler. I would make Ava maybe draw a picture or something and then we’d hang it near his cot by the nursery. So she felt important. The nurses would get involved and go, oh Ava, did you do this, and she goes, yes, this is for my baby brother, and she’d be a part of it too. Just even heating up a little bottle, come on Ava, let’s go heat up Tyler’s bottle, she’d come with me. Then also it’s normal for her too, because then she’s not scared of it, because you’re introducing this all to her, which is funny – when he does rip out the tubes, she goes, oh Tyler, now we have to go to the hospital. She’s a part of it. Oh Tyler, you silly boy, and then starts telling him like that. Which is like, it’s cute and funny and all that. She understands the process of it all.”
Gina
Gina
Kitty described how her older boy was involved in feeding his younger brother. Just like with Gina and her kids, it was about finding a way for the siblings to feel involved and helpful:
“Whenever Luke asked, what’s that, we explained it to him. Then when we went home, when I would feed, he’d pass me the syringe, or I’d get him to pass me some of the things. So he was part of the feed as well. But also, he knew for example, if Geoffrey rolled on his tube and it’s behind him and it’s pulled or something, he would call me automatically. Or if he knew, for example, if the tube was – as he got older, what he would do is, if the tube was in a position where it’s going to get caught, he would just move it a little bit. But he’ll ask me as well and I would say, yes. If he takes even – but that’s with everything, even if he took off his helmet for his head, he would come and call me straightaway. It sort of – it’s funny, but they’re aware.”
Kitty
Kitty
Balancing your attention
Jess explained why this is hard, and the strategies she and Guy used to help their son Nick feel he got enough loving attention, without compromising the extra care that Amanda needed given her feeding difficulties
Click here to read more…
“I think the biggest thing for us was we didn’t want him to be jealous of his sister.”
Guy and Jess
What Guy and Jess felt was shared with many other parents of tube-fed children who had other brothers or sisters. Jess explained why this is hard, and the strategies she and Guy used to help their son Nick feel he got enough loving attention, without compromising the extra care that Amanda needed given her feeding difficulties.
“I never wanted Nick to feel left out or jealous. Because at the end of the day, when you have a sick kid, a lot of your attention is on that kid. You feel bad as well. As a parent, I felt like I’m not spending enough time with him. So I made sure at that point as well, is that first, I paid attention to him. Second is he had his grandparents around him. While I’m spending that time with Amanda, I had them spending some time with him as well, because I can’t give him the full attention. He loves going there now. But also with Guy, what we did was he said, you focus on the little one and I’ll focus on Nick. We split our focus and that way they’ve both got enough attention. I think the biggest thing is, if both parents are focussing on that little sick kid, then the other one is left out. I think that’s when they start to get jealous and they’re playing up and they’re wanting your attention and all that. But we still gave them both attention. I think that’s the biggest thing, don’t forget about your other child.”
Guy and Jess
Guy and Jess